 Geostrategic Media Political Commentary, Analysis, Security, Defense
Geostrategic Media Political Commentary, Analysis, Security, Defense

Giancarlo Elia Valori
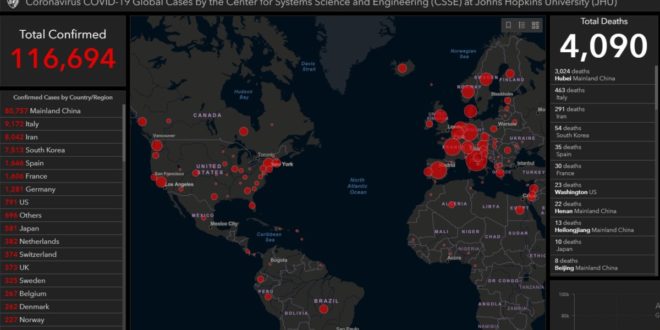
The economic data linked to the mass infection by Covid-19 is already very alarming.
The Italian public health system, along with many other primary sectors of public spending, has already bore the brunt of budgetary restrictions.
Currently, the deficit we record in relation to the needs resulting from the Covid-19 infection s to over 10 billion euros compared to current standard needs.
In Italy there are 5.5 nurses per thousand inhabitants, while in the United Kingdom they are 7.9, in France 10.5 and in Germany 12.6.
According to our nursing associations, in Italy there is already a shortage of 50,000 nurses compared to the initial standard of service.
As many as 70,000 beds have been eliminated, just when the Italian population is ageing, and there is a lack of at least 8,000 general practitioners.
According to the Northern Regions, however, the situation is far more alarming: there is a lack of at least 35,000 doctors and some Regions have already called back into service retired doctors and young doctors who have not yet completed their specialization.
The doctors still at work, however, are aged 52 on average and hence they will retire shortly.
The Veneto region alone has a shortage of as many as 1,300 doctors.
The healthcare staff in Lombardy and in the other regions already hit by the Covid-19 infection has not been resting for a long time: they work in the normal daily shifts and then, at night, they are on call. This often means very hard work.
Hence we can easily imagine the mental stress, the nervousness, the lack of rest and the residual concentration of these doctors, who are always very cooperative.
According to Bocconi’s CERGAS, the scientific observatory on healthcare economics in Italy, between 2012 and 2017, 759 hospital wards were abolished (5.6%), while there are still 3.2 beds per thousand inhabitants, compared to 6 in France and 8 in Germany.
Almost all the “small hospitals” – which, for some reason, are always considered useless spending centres by the so-called experts of the Regions and the Health Ministry – have been closed, thus putting in crisis the major hospitals, already overburdened both in terms of therapies and beds.
Furthermore, Italy has 20% of financial resources available in healthcare compared to Great Britain – which also had to face Thatcher’s anti-State policy of drastic spending cuts – 34% less than France and even 45% less than Germany.
Why these shortages of funds? For the spasmodic implementation of “spending cuts” to be shown to the EU, like good schoolchildren.
What if we said at EU level that health spending should be outside the checks on the notorious 3% ceiling, a percentage superficially invented at the time by an expert, just to write something?
In short, every year the Italian State spends 119 billion euros on public healthcare, but our fellow countrymen pay additional 40 billion euros from their own pocket, through co-payments, etc.
The effects can be seen.
In Milan the waiting time for a surgery is nine months and it should also be recalled that the Covid-19 infection requires that the few resources still available are used to bear the immediate costs for the adaptation of health facilities to the coronavirus emergency.
Nevertheless, the shortcomings persist: since 2010, in Italy, there has been a lack of 5.4% doctors, of 4.3% nursing staff and of 9.1% other staff.
The miracle is that, even today, everything is working at its best, thanks to the quality and professionalism of the people operating in the Italian healthcare sector.
Whoever experiences a health system like Italy’s, does not forget it. Just recall the case of Mark Hinkshaw, or of the American writer who was saved by the doctors of the Cardarelli hospital in Naples and told her story it in an article in the New York Times.
Now, however, there is a problem. How can we increase funding for the Italian National Health Service (NHS) without exceeding the budget ceiling that the EU authorities impose on us?
Currently the funding sources for Italy’s NHS are the health units’ own revenue, i.e. co-payments or intramoenia revenue; the Regions’ general taxation, i.e. the Regional Tax on Productive Activities (IRAP) – as is already provided for its healthcare share – and the additional regional tax to IRPEF, i.e. the personal income tax.
If the amount of these taxes or fees is lower than the minimum calculated on an historical basis, there will be the supplement of the Guarantee Fund pursuant to Article 13 of Legislative Decree 56/2000.
As to the healthcare share, the resources coming from IRPEF and IRAP are paid to the Regions on a monthly basis.
The State Budget finances what remains unpaid by the National Health Service, through the co-payment and sharing of Value Added Tax (VAT) and through the National Health Fund.
In 1980 the NHS cost 9.3 billion lire and accounted for 4.7% of GDP. Currently it costs 117 billion euros and accounts for 6.8% of GDP.
If this continues, the NHS shall be privatised, to the delight of insurance companies, which are floundering in a commercial crisis and are looking for other business, as well as the private healthcare sector which, however, paradoxically, is mainly funded by the public.
Clearly the NHS privatisation is the ultimate goal of many politicians and lobbies.
With the increase in poverty, in Italy, this would be the recipe for an unprecedented social clash.
Nowadays the NHS is funded by general and regional taxation, but IRPEF and IRAP are always insufficient, like VAT. It is also funded by regional taxation itself, i.e. the transfer of the health cost burden from companies to households (due to the crisis, the IRAP share decreases), and by the now long-standing deficit spending.
The first (fiscal) consolidation took place in 2006 and the NHS has already accumulated debt for a nominal value of 98.9 billion euros, equal to 149.4 discounted.
Hence what can be done to rescue all the social healthcare facilities? Considering UK Prime Minister Johnson’s latest proposals, a medium-term debt instrument dedicated to healthcare may be issued both in Italy and Great Britain. Currently the securities market is dominated by a very low average interest rate. Probably it is time to try.
Or the systems may be integrated, by proposing the exchange of doctors, nurses, but above all patients, between the two countries. With a non-monetary calculation of expenses. This will be the core to preserve public health in Europe or in the European civilized countries.
GIANCARLO ELIA VALORI
Honorable de l’Académie des Sciences de l’Institut de France
President of International World Group
March 2020



